Erginus sybaritica (Dall, 1871)
(Figs. 20 a-f)
External Anatomy: Mantle margin with crowded series of minute circumpallial tentacles in living animal, which are completely retracted when preserved. Attachment of shell muscle horseshoe-shaped, divided into about fourteen segments by vessels. Thin pallial muscle connecting anterior ends of shell muscle. Head provided with pair of non-papillate cephalic tentacles with invaginated eyes on their outer bases. Outer lip of mouth with laterally swollen oral lappets. Prominent subcephalic tentacle (sct) beneath right cephalic tentacle (Figs. 20 a, b), with surface entirely covered by dense cilia (Figs. 20 c, d). Internally, tentacle with muscular fibers, narrow blood space, and nerve from right cephalic ganglion, without tubular duct-like structure. Sensory projections and pallial streaks absent in pedal region.

Pallial Complex: Pallial cavity relatively deep, attaining nearly half of body length, containing paired kidney openings and anus, but lacking ctenidium, osphradium, and hypobranchial gland. "Secondary gills" also absent. Pallial cavity deeply developing into brooding chamber during breeding season.
Digestive System: Oral region provided with inner lips associated with transverse labial muscles and anterior wings of jaw. Oral tube not clearly surrounded by buccal sphincter and constrictor. Muscles of odon-tophore consisting of dorsal protractors, lateral protractors, ventral protractors, and anterior levators. Depressors and levators absent in posterior part. Dorsal and postdorsal buccal tensors also absent.
Jaw consisting of small anterior wings, large posterior wings, and medially thickened smooth anterior band. Anterior part of jaw covering oral tube; posterior wings with connection to anterolateral projections of cartilages.
Radular sac forming single loop in visceral mass; posterior end inflated with development of odon-toblasts, but not bifurcated. Radula formula 0-3-0-3-0 (Fig. 20 f). Radular row symmetrical. Three lateral teeth arranged in inverted V-shape. Innermost laterals with blunt cusp and longest base. Middle laterals situated posterolaterally to innermost; cusp blunt and elongate. Outermost laterals fused anterolaterally with middle teeth; cusp blunt, triangular, with outward lateral projection. Basal plates thick, wider than long, with smooth surface.
Muscles of subradular membrane consisting of lateral protractors, median protractors, and retractors of subradular membrane. Median protractors not asymmetrical. Retractors not fused ventrally. Muscles of radular sac composed of retractors of radular sac. Both median retractor of radular sac and ventral tensor of radular sac absent.
Buccal mass containing two pairs of cartilages: anterior and anterolateral. The former connected by two-layered ventral approximator. Sublingual pouch deep, simple, without projections of sublingual gland. Licker smooth in macroscopical observation, but with microprojections in transverse arrangement under SEM observation (Fig. 20 e). Radular diverticulum widely developed, depressed over odontophore.
Salivary glands not well developed, elongated longitudinally on outer posterior sides of buccal mass. Paired salivary ducts running along anterior esophagus from anterior ends of salivary glands to lateral extensions of buccal cavity.
Anterior esophagus provided with inflated dorsal food channel and depressed lateral pouches, internally divided by conspicuous dorsal and ventral folds. Mid-esophagus partitioned by lamellate projections. Posterior esophagus narrow, longitudinally corrugated internally. Stomach C-shaped, simple in internal structure; gastric caecum, tooth of gastric shield, and corrugated sorting area absent. Intestine with four complex loops. Rectum (fourth loop of intestine) not penetrating pericardium or ventricle, directly contacting posterior pericardial wall in non-breeding individuals due to reduction of gonad.
Circulatory System: Heart consisting of single auricle and ventricle. Auricle laterally elongated, connected with efferent pallial vessel in left comer and with numerous capillary vessels from nuchal cavity roof throughout anterior margin. Ventricle posterolaterally elongated, connected with auricle anteriorly, leading into bulbous aorta ventrally. Pericardium heavily compressed posteriorly with development of nuchal cavity as brooding pouch.
Excretory System: Asymmetrically paired kidneys present. Left kidney much smaller than right, extremely elongated along left side of rectum. Left kidney opening narrow and simple. Right kidney widely spreading over base of visceral mass, distinguishable from visceral organs by yellowish hue in living animal. Right kidney opening prolonged as very thin tube. Left renopericardial canal extending along posterior limit of pallial cavity; right renopericardial canal could not be confirmed.
Reproductive System: Gonad widely spreading below digestive glands, with thin connective duct to right kidney. Hermaphroditism not confirmed. Relatively large, few eggs directly deposited in nuchal cavity. As eggs develop, nuchal cavity becoming enlarged as brooding pouch to accommodate juveniles, pushing visceral region backward.
Nervous System: Configuration of ganglia and nerves similar to that in Niveotectura.
Erginus moskalevi (Golikov and Kussakin, 1972)
(Figs, 21 a-c)
Protoconch: Protoconch symmetrical, oval, shield-shaped. External surface sculptured by tiny pits, each 1.25-5 p-m in diameter (Fig. 21 c). Protoconch-teleoconch boundary clearly demarcated by abrupt change in sculpture; exterior surface of early teleoconch finely punctate. Protoconch situated in symmetrical position relative to sagittal axis of teleoconch. Young snails brooded in pallial cavity of parent, remaining there until at least 460 µm in shell length. In brooded condition intact protoconch still retained; septum beginning to seal inside of apex. Inside of protoconch and early teleoconch seem to have small shell pores not found in adult shell.
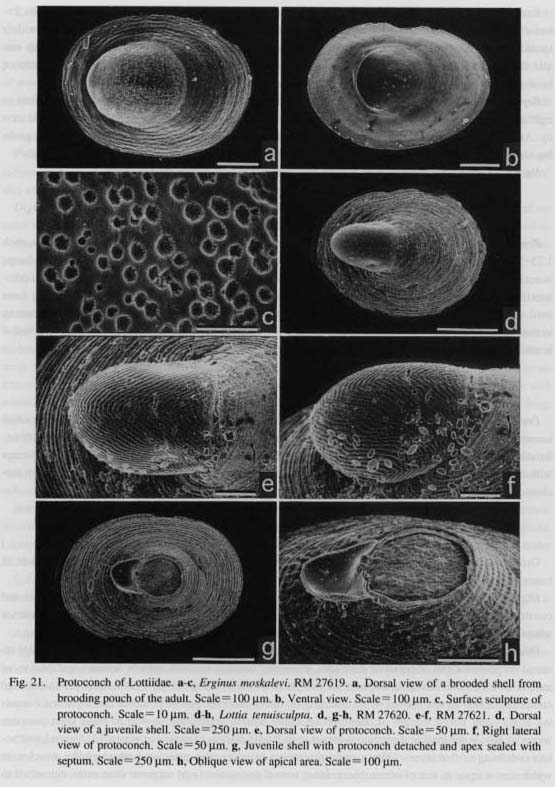
Lottia tenuisculpta Sasaki and Okutani, 1994
(Figs. 21 d-h)
Protoconch: Protoconch symmetrically elongated, cup-shaped, lateroventrally inflated, exhibiting small constriction and slight lateral extensions (so-called lateral pouches). Outer surface entirely covered with undulating striae. Apertural lip of protoconch nearly straight. Protoconch generally lost at very early stage with shell length of 0.5-1 mm after inside of apex sealed off by septum, easily detached from apex by mechanical shock.
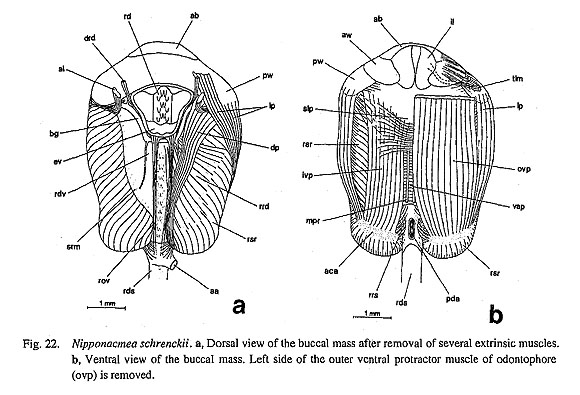
Nipponacmea schrenckii (Lischke, 1868)
(Figs. 22 a-b)
Gross anatomy of this species described by Sasaki and Okutani (1993 a). Additional observations on buccal mass described below.
Digestive System: Oral tube dorsally covered by jaw, not clearly surrounded by buccal sphincter and constrictor. Inner lips linked with transverse labial muscles (tarn) running along inner sides of anterior wings toward lateral walls of snout (Fig. 22 b).
Odontophore fixed on body wall by following four muscles (Figs. 22 a, b): (1) Dorsal protractors (dp) inserted on posterior end of posterior cartilages, extending forward between anterior levators and dilators of radular diverticulum, attaching to posterior margin of posterior wings of jaw. (2) Lateral protractors (lp) composed of two layers, both of which inserting on lateral posterior end of posterior cartilages and extending along outer lateral margin of odontophore. Outer muscle originating in wall of snout over posterior wings of jaw; inner muscle directly connected with lateral margin of posterior wings. (3) Ventral protractors consisting of two layers. Outer ventral protractors (ovp) as most prominent odontophoral muscles; in width almost equal to that of odontophore. Inner ventral protractors (ivp) narrower than outer, connected to posterior cartilages and ventral surface of sublingual pouch. Anteriorly right and left sides linked with transverse Sheet of muscle. (4) Anterior levators (al) inserted on outer sides of anterolateral cartilages, ex
tending dorsally beneath labiobuccal connective, attaching to origin of dorsal wall of snout. Depressors and levators absent in posterior part.
Muscles of subradular membrane consisting of three pairs: (1) Median protractors of subradular mem brane (mpr) very thin, symmetrically positioned. (2) Lateral protractors (lpr) much thicker than median pairs. (3) Subradular membrane affixed to odontophore by retractors of subradular membrane (rsr), clearly divided into pair, not fused ventrally.
Radular sac pull only by retractors of radular sac (rrs) running between ventral side of radular sac and posterior cartilages. Both median retractor of radular sac and ventral tensor of radular sac absent.
Odontophoral cartilages consisting of elongated anterior and triangular anterolateral cartilages. Anterior cartilages medianly connected by ventral approximator muscle. Labial cartilages (as in Celland) absent.
Family Pleurotomariidae Swainson, 1840
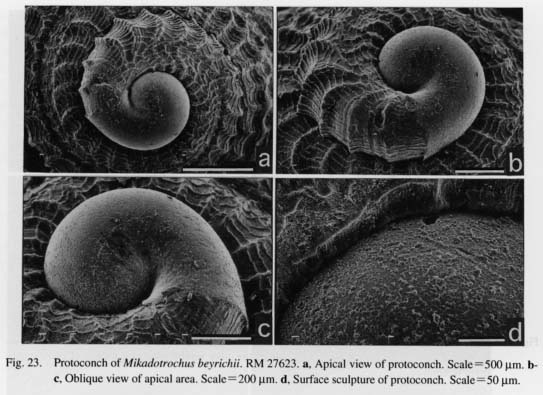
Mikadotrochus beyrichii (Hilgendorf, 1877)
(Figs. 23 a-d, 24 a-b, 25 a-d, 26 a-d, 27 a-h)
Protoconch: Protoconch tightly coiled in 1.25 whorls, its direction slightly hyperstrophic against teleo-conch (Figs. 23 a-c). Observed shell empty and eroded, with irregular fine granulous deposits and two fine spiral threads clearly visible in apical view (Figs. 23 c-d). Protoconch-teleoconch boundary marked by abrupt appearance of spiral riblets on teleoconch. Slit not formed in protoconch but inserted between spiral riblets in early teleoconch (Fig. 23 a).
External Anatomy: Animal trochiform. Mantle deeply sinuate in midline (Figs. 24 a, b). Mantle margin (mm) divided into two folds by periostracal groove (pg) (Fig. 27 b). Outer fold (of) smooth, sharply edged. Inner fold (if) thicker than outer, provided with several layers of densely overlapping microtentacles. Inner surface of inner fold finely denticulated by longitudinal furrows (Fig. 24 b). Attachment of columellar muscle (cm) restricted to narrow subrectangular area. Muscle not divided into bundles.
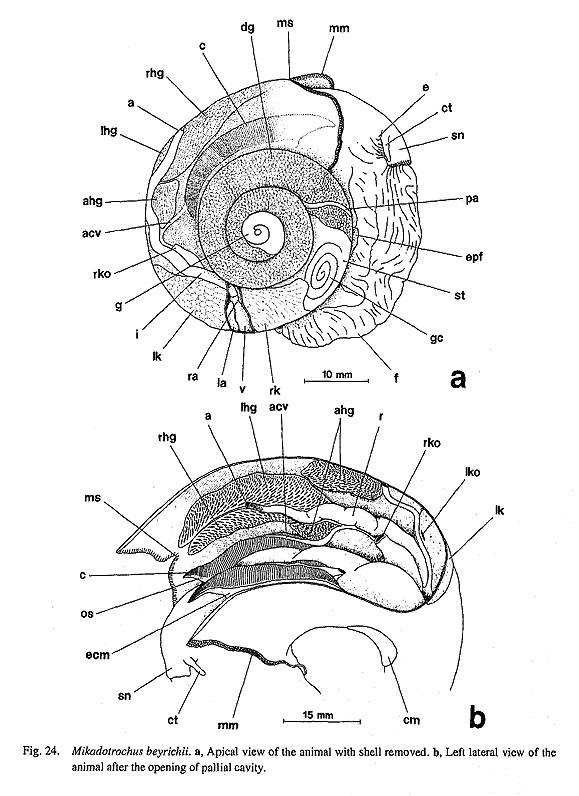

Head with cylindrical snout (sn), and pair of thick cephalic tentacles (ct) without papillae. Cephalic lappets absent. Outer lip (ol) thickened as oral disk, covered by numerous papillate projections (Fig. 25 b). Eyes open, at bases of cephalic tentacles, without eyestalks. Inner layer of retina containing tall black pigmented cells.

Foot (f) very large, inflexible, folded longitudinally (rather than anteroposteriorly) when retracted. Epipodial region comprising several (3?) pairs of epipodial flaps (epf) (Fig. 24 a). Ventral margin of flaps fringed by tuberculate microprojections, which presumably represent epipodial sense organs (Fig. 27 c).Posterior side of epipodium with multispiral operculum. Attachment for operculum thickened, reflected as opercular lobe. Surface of head-foot region somewhat papillate, covered by layer of tall columnar cells (Fig. 27 a).
Pallial Complex: Pallial cavity very deep, occupying one-half volution of body whorl, including paired ctenidia, paired osphradia, paired kidney openings, anus, and paired hypobranchial glands (Fig. 24 b). Organs of columellar side slightly shorter than those of peripheral side.
Ctenidial lamellae bipectinate. Efferent ctenidial axes attached to outer ventral sides of pallial wall by long efferent ctenidial membranes (ecm); afferent sides totally lacking membrane connecting to mantle. Both ctenidial axes containing well expanded ctenidial vessels, nerves, and paired retractor muscles. Free portions of afferent axes also bearing skeletal supports. Each lamella elongated triangular, with tip of terminal ridge directed toward inside, stiffened by skeletal rods, with surface of zones of cilia. Bursicles evidently lacking on efferent sides of leaflets; no trace of knobby structures or associated grooves of typical bursicles in SEM observation (Fig. 27 d).
Osphradia (os) situated at free portions of efferent ctenidial axes, paired in agreement with ctenidia (Fig. 27 d). Surface of osphradium sporadically covered with cilia (Fig. 27 e).
(rhg, lhg) by rectum in posterior half. Each paired gland with accessory lobe posteriorly (ahg, Fig. 24 b), structurally identical in having network of vessels and glandular epithelium (Fig. 27 f). Both main and accessory glands somewhat reduced on right side.
Digestive System: Oral tube surrounded by buccal sphincter and constrictor (bs, bct) with mandibular protractors and retractors (mp, mr). Buccal mass fixed by lateral protractors (lp), outer and inner ventral protractors (ovp, ivp), anterior levators (al), posterior depressors (pd), and dorsal buccal tensors (dbt) (Figs. 25 a-c). Posterior part of odontophore tightly bound by thick band of postdorsal buccal tensor (pdt). Dorsal buccal tensors (dbt) consisting of outer and inner parts: outer part connecting to buccal constrictor, inner part uniting with dorsal wall of snout. Separate levator muscles absent; outer part of lateral protractors probably providing antagonistic function for depressors.
Paired jaws projecting from dorsal side of oral tube. Very characteristically, entire jaw plate fleshy, not cuticularized; surface and anterior margin completely smooth.
Radular sac rather long along right side of mid-esophagus, straight in configuration. Surface surrounded by thick connective tissue of radular artery. Posterior end deeply bifurcated. Radular formula roughly ca. 60-ca. 40-1-ca. 40-ca. 60, but tooth arrangement cannot be exactly categorized because of aberrant derivation. Radula divisible into inner central tooth field with shorter teeth and outer marginal field with longer teeth. Each transverse radular row symmetrical in marginal tooth fields but clearly asymmetrical in central tooth field. Central tooth elongated, with thin shaft, without cusp; outline of shaft and base distorted by asymmetry together with several neighboring teeth. First and second pairs of lateral teeth especially filamentous, undulate, skewed to either right or left, greatly asymmetrical. Following teeth lamellate, with inverted V-shaped configuration. Within inner zone of marginal fields, teeth elongated with sickle-shaped cusps; teeth becoming shorter toward outside, with tip of cusp acutely pointed in spinous form; pointed cusp divided into three branches, with dorsal side giving rise to filaments. Outermost teeth smooth, lacking projection or filamentous structure.
Subradular membrane inserted by median and lateral protractors (mpr, lpr) and retractors of subradular membrane (rsr). Radular sac pulled back by retractors (rrs) originating from posterior odontophoral cartilages and by postmedian retractors of radular sac (prs) from floor of body cavity. Thin tensor muscle (trs) arising from dorsal side of sublingual pouch, extending in median line backward, ending behind insertion of postmedian retractors.
Odontophore containing two pairs of cartilages (Fig. 25 d). Anterior cartilages (aca) longitudinally elongated with weak anterolateral extension. Posterior cartilages (pca) much smaller than anterior, attached to posterior end of anterior cartilages ventrally. Anterior pair of cartilages united by ventral approximator (vap). Anterior and posterior pairs longitudinally connected by outer approximators (oap) on outer sides.
Sublingual pouch (slp) not generating glandular outgrowth (Fig. 25 b). Licker (lic) thickened on anterior part of subradular membrane. Salivary glands (sg) spreading over buccal cavity, discharging into it through longitudinally slit-like openings without ducts. Surface of glands split into numerous minute branches. Inner margin of opening of salivary glands (sgo) especially thickened (Fig. 26 b).

Anterior esophagus expanded laterally to form esophageal pouches (ep) that enclose greater posterior part of buccal mass except ventral side. Dorso ventrally depressed lateral pouches not formed. Saclike projection formed posterior to esophageal valve (ev) over radular diverticulum (Fig. 26 b). Interior of esophageal pouches and entire midesophagus lined with glandular epithelium with long papillate projections. Midesophagus (me) extremely elongated, as long as one-half volution of body whorl (Fig. 26 a). Dorsal folds (df) fused into broad band; similarly paired ventral folds (vf) united into single fold over buccal mass. Both folds gradually twisted counterclockwise in mid-esophagus. Posterior esophagus (pe) distinctly constricted, much shorter than mid-esophagus.
Stomach (st) strongly bent, divided into proximal and distal regions (Fig. 26 c). Spiral gastric caecum
(gc) prominently developing on dorsal surface. Most of stomach occupied by smooth-surfaced gastric shield (gs). Tooth of gastric shield not found. Ridge-like structures rather unclear throughout interior of stomach: partition of sorting area (sa) not very apparent; two ridges continued into spiral caecum until they disappear near tip of caecum. Digestive glands opening by two distantly separated openings (dgo). Posterior (topologically anterior) opening leading to dorsal lobe of glands, while anterior (topologically posterior) opening connecting with ventral lobe. From right side of posterior digestive opening, major and minor typhlosoles (mt, nt) extending into intestine. Intestinal groove (ig) between two typhlosoles very broad.
Intestine (i) running forward along right side of body wall, bending back to trace same course on left side, forming single very long anterior loop (Fig. 26 a). Intestine then curving dorsally, penetrating pericardium and ventricle, entering pallial cavity. Rectum running along mid-line, ending at anus (a) at anterior two-thirds of pallial cavity.
Circulatory System: Pericardium on posterior side of left kidney (Fig. 24 a). Heart consisting of smaller right and larger left auricles and single ventricle. Left auricle (la) on anterolateral side of ventricle; right one (ra) on posterolateral side.
Aorta divided into anterior and posterior aortae within pericardium. Aortic bulb indistinct. Posterior aorta (pa) transporting blood to stomach and digestive glands. Initial part of anterior aorta running within mantle skirt, near posterior end of ctenidium, bending to lead into anterior visceral region along esophagus. In head region, aorta opening into cephalopedal sinus through buccal and pedal arteries. Radular sac enclosed posteriorly by radular artery.
Excretory System: Two greatly asymmetrical kidneys on posterior and anterior sides of pericardium (Fig. 24 a). Right kidney (rk) much larger than left; its inner wall attached by fenestrated lamellae; its posterior lobe exposed on dorsal surface posterior to pericardium; anterior lobe deeply spreads over right side of anterior visceral region (Fig. 27 g). Terminal part near right kidney opening especially enlarged to form long tube of urogenital papilla (Fig. 24 b), but histological nature (pallial origin?) not observed. Presence of sexual dimorphism in terminal part not verified because of immaturity and incompleteness of available individuals. Right renopericardial duct opening to pericardium beneath right auricle.
Left kidney (lk) lying within pallial cavity, overhanging pallial roof, its inner wall covered by papillate projections, being shorter in anterior section but longer in posterior (Fig. 27 h). Slit-like left kidney opening (lko) lying on inner anterior side of kidney (Fig. 24 b). Left renopericardial duct opening near right limit of left auricle.
Reproductive System: Structure of reproductive system not adequately determined because gonads of available specimens were immature or visceral hump was torn off within upper whorls of shell.
Nervous System: Circumesophageal nerve ring basically hypoathroid (Fig. 26 d). Cerebral ganglia (cg) well developed at bases of cephalic tentacles. Pleural ganglia (plg) on outer anterior sides of pedal ganglia, completely fused with pedal ganglia. Characteristically, cerebropleural and cerebropedal connectives (cpc, cdc) with fused origin at their base.
Cerebral ganglia laterally emitting tentacular and optic nerves (tn, opn). Inner anteroventral sides innervating labial region. Ganglia dorsally connected to cerebral commissure (cc) which gives rise to fine nerves toward oral tube. On ventral side, labial ganglia and commissure absent. Cerebrobuccal connectives (cbc) arising from inner ventral sides of cerebral ganglia. Buccal ganglia (bg) lying over odontophore, innervating entire buccal musculature, anterior esophagus, radula, and associated structures.
Visceral loop originating (unusually) from cerebropleural connectives (cpc), rather than directly from pleural ganglia (Fig. 26 d). Supraesophageal part of loop (spv) on right side arising from nearer anterior end than subesophageal part (sbv) of left side. Cerebropleural connectives running more dorsally than cerebropedal connectives (cdc), being pulled up by initial parts of visceral loop. Visceral loop extremely long, correlating with depth of pallial cavity. Ganglionation of supraesophageal, subesophageal, and visceral sections all indistinct, and therefore loop seems to be of simple cord-type throughout its length. Nerves originating from sub and supraesophageal parts to osphradio-ctenidial ganglia (osg), kidneys, rectum, and pericardium.
Pedal cords (pcd) exhibiting well-developed, ladder-like configuration. At least sixteen distinct pedal commissures between pedal cords toward posterior end of foot (Fig. 26 d). Disposition of commissures not always parallel, their thickness also varying slightly. Pedal cords also with thin pedal or epipodial nerves on each outer side. From anterior sides of pedal ganglia, more or less thick pair of anterior pedal nerves extending into pedal musculature. Statocysts lying on anterodorsal sides of pedal ganglia.
Family Haliotidae Rafinesque, 1815
Sulculus diversicolor aquatilis (Reeve, 1846)
(Figs. 28 a-d, 29 a-b, 30 a-b, 31 a-f, 32 a-d, 33 a-b)
Protoconch: Protoconch planispirally coiled, inrolled by early teleoconch (Figs. 28 a-b). Neither lateral pouch nor suture ofprotoconch clearly formed; only slight constriction in center representing trace of spiral coiling. Sculpture on protoconch consisting primarily of irregular deposits with round pits and several spiral lirae that develop subtly (Figs. 28 b-c). Boundary between protoconch and teleoconch marked by simple axial line (Figs. 28 d).

External Anatomy: Animal markedly depressed dorsoventrally with small spiral viscera] hump. Mantle deeply sinuated along midline of pallial cavity (Figs. 29 a, b). Mantle margin (mm) lacking circumpallial microtentales; three long pallial tentacles (pt) projecting from mantle margin. Median one arising from posterior end of mantle slit; anterior two lying over head region anteriorly. Left tentacle situated slightly anterior to right one.
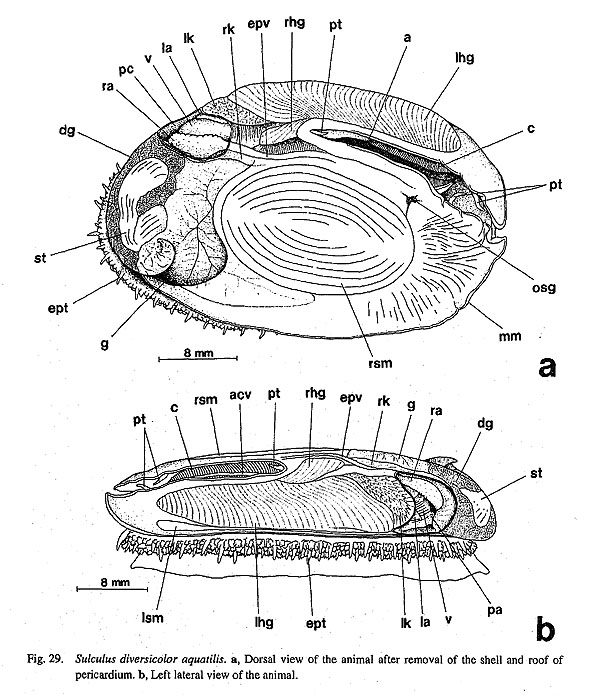
Shell muscles composed of paired muscles of extremely unequal size. Right shell muscle (rsm) large, oval, in center of body. Left muscle (lsm) thinly elongated below anterior part of left hypobranchial gland, not visible from dorsal side.
Head provided with papillate cephalic tentacles (ct), eyestalks (es), and cephalic lappets (clp). Cephalic lappets fused with each other in midline and also with inner margin of eyestalks, extending over bases of cephalic tentacles. Eyes open, filled with vitreous body at tip of eyestalks. Neck lobes absent.
Foot very large, reaching almost entire body length. Epipodium circularly fringed by epipodial tentacles (ept), consisting of long papillate and short dendritic tentacles. Epipodial sense organs present only at bases of long tentacles, taking form of simple ciliary tuft. Operculum absent.
Pallial Complex: Pallial cavity very deep, reaching two-third of body length, containing paired ctenidia with osphradia, paired kidney openings, anus, and paired hypobranchial glands.
Paired bipectinate ctenidia (c) in pallial cavity in slightly asymmetrical arrangement (Fig. 30 a). Efferent ctenidial axes fixed on pallial wall by long efferent membranes (ecm) except at free anterior portion. Afferent side entirely lacking afferent membrane, Ctenidial axes containing well-developed efferent and afferent ctenidial vessels (ecv, acv), nerves, and paired retractor muscles. Free portion stiffened by skeletal rods.
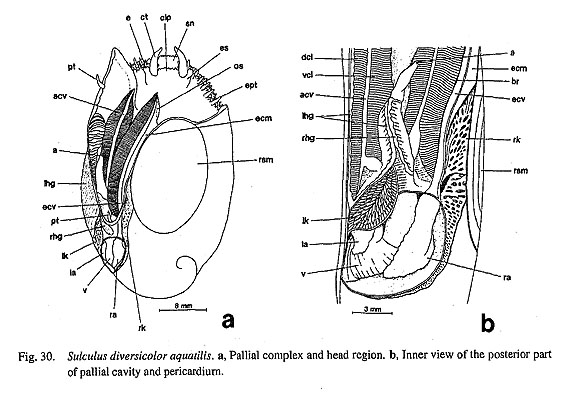
Ctenidial lamellae depressed, triangular, with three zones of cilia on exterior surface and skeletal rods at efferent sides internally. Efferent sides of both dorsal and ventral lamellae (del, vcl) with longitudinal row of bursicles (br) near efferent axes.
Osphradial epithelia covering free portions of efferent ctenidial axes (os, Fig. 30 a). No distinct zonation observed on outer surface; surface sparsely covered with cilia in SEM observation.
Hypobranchial glands attached to roof of pallial cavity. Right and left glands greatly unequal in size. Right gland (rhg) lying in posterior end of mantle cavity over rectum. Left gland (Ihg) elongated anteriorly along left pallial cavity wall, finely branched into many transverse sections by pallial vessels, with inner wall prominently lamellate. Right and left glands in contact with each other over midline of rectum.
Digestive System: Oral tube surrounded by thick layers of buccal sphincter and constrictor (bs, bet) with mandibular protractors and retractors (mp, mr). Buccal mass fixed on body wall by lateral protractors (lp), outer and inner ventral protractors (ovp, ivp), anterior levators (al), posterior levators (pl), posterior depressors (pd), and dorsal buccal tensors (pdt) (Figs. 31 a, b). Lateral and ventral protractors elaborated into especially thick muscle strands, but posterior pairs of depressors and levators much thinner than protractors. Posterior levators arising from inner ventral end of posterior cartilages, crossing under posterior depressors. Anterior levators located outside of inner part of lateral protractors, but inside of outer part of lateral pro
tractors and dorsal buccal tensors. Paired odontophoral cartilages fixed by postdorsal buccal tensor. Dorsal buccal tensors (dbt) running within space between outer and inner parts of lateral protractors, attached to anterolateral extensions of anterior cartilages.
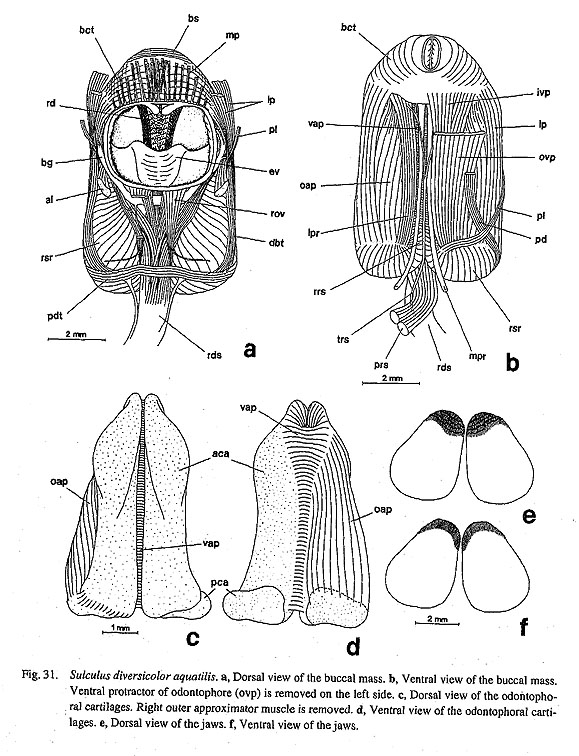
Jaws (j) separated into distinct pair (Figs. 31 e, f). Anterior margin fimbriate, with fine chitinous rods denser on dorsal side than on ventral side. Posterior two-thirds of jaw attached to wall of oral tube, while remaining anterior section free from oral cavity.
Subradular membrane controlled by lateral and median protractors (lpr, mpr) and retractors (rsr). Median pair attaching to floor of body wall behind buccal mass, while lateral pair inserting on posterior cartilages. Radular sac pulled back by retractors (rrs) within odontophore and by postmedian retractors (prs) behind odontophore. Very thin tensor muscle (trs) running medially from site near sublingual pouch to ventral side of radular sac behind buccal mass: its anterior portion bifid; its posterior end running to right side of postmedian retractors, not between them.
Radular sac straight in configuration, attaining half of body length. Posterior end of radular sac deeply bifurcated. Radular formula n-5-1-5-n (Figs. 32 a, d). Transverse radular row asymmetrical; left side skewed more anteriorly than right. Central tooth with broad trapezoidal base and non-denticulate cusp; form of tooth itself symmetrical, but its disposition skewed asymmetrically toward left. Inner two pairs of lateral teeth also constituting central tooth field that has spacious zone of short-stalked teeth. First laterals also oblong; its width almost equal to that of central tooth. Second laterals situated more anteriorly, smaller than first laterals. Outer three laterals much more elongated than inner two; third teeth largest in radular row. Lateromarginal plates absent. Marginals with thin elongated shafts and finely serrated cusps.

Odontophore supported by two pairs of cartilages (Figs. 31 c, d). Anterior cartilages (aca) longitudinally elongated with anterolateral extensions; anterior tip forming hook ventrally. Posterior cartilages (pea) attached to posterior end of anterior cartilages ventrally and projecting laterally. Median side of anterior pair connected by ventral approximator (vap). Anterior and posterior pairs united by outer approximators (oap).
Sublingual pouch represented by shallow simple sac. Smooth licker clearly formed on anterior end of subradular membrane. Radular diverticulum deep below well-developed esophageal valve. Salivary glands (sg) spreading over roof of buccal cavity, discharging directly through longitudinal slits. Surface of salivary glands finely ramified by vermiform outgrowths.
Anterior esophagus terminating over buccal mass. Inner wall of esophageal pouches (ep) and midesophagus (me) extensively covered with papillate projections of glandular epithelium. Ventral folds fused in middle part; dorsal folds running independently through mid-esophagus. Both ventral and dorsal folds progressively twisting counterclockwise inside mid-esophagus. Posterior esophagus (pe) characterized by reduction in diameter and by many longitudinal grooves.
Stomach (st) strongly folded into proximal and distal regions near apex of visceral mass (Figs. 33 a, b). Distal part bending anteriorly along left margin of proximal part. Dorsal side of folded region bearing large spiral gastric caecum (gc). Ducts from digestive glands (dgo) opening on floor of proximal region and inner dorsal side of distal region. Internally, pair of longitudinal folds continuing to interior of spiral caecum. Ciliated sorting area (sa) between two folds exhibiting transversely corrugated sculpture. Tooth of gastric shield (gst) lying on posterior wall of gastric shield. Intestinal groove on ventral side marked by major and minor typhlosoles (mt, nt) toward intestine. Protostyle (formed by consolidation of gut contents in rod form) contained in distal region and initial part of intestine.

Intestine passing over stomach, extending anteriorly beside shell muscle, reaching buccal region to form long anterior loop that partly overlaps right esophageal pouch (Fig. 33 a), following same course in opposite direction, bending to penetrate pericardium and ventricle, finally ending anteriorly as anus. Within pallial cavity rectum attached to right and left hypobranchial glands posteriorly, but remaining anterior part freely projecting within the cavity.
Circulatory System: Pericardium lying on posterior side of pallial cavity. Heart consisting of large right auricle, small left auricle, and median ventricle (Fig. 30 b).
Venous blood from kidneys entering expanded space at bases ofctenidia (basibranchial sinus). Right and left sides of sinuses communicating beneath rectum, followed by afferent ctenidial vessels (acv). Blood passing through ctenidial lamellae entering efferent ctenidial vessels (ecv) together with those transported via pallial and hypobranchial vessels, draining into auricles. On left side, efferent renal vessel from left kidney joining before entering auricle.
Excretory System: Excretory system consisting of paired but greatly asymmetrical kidneys (Fig. 30 b). Right kidney (rk) developed along right posterior parts of pallial cavity and pericardium, also widely spreading toward anterior visceral region over intestine. Lumen spacious, inner wall partitioned by perfo rated lamellae. Left kidney (lk) much smaller than right kidney, lying on anterior left side of pericardium. Inner wall thickly covered with finger-like projections representing so-called papillary sac. Each kidney with renopericardial duct.
Reproductive System: Gonochoristic gonad (g) situated over digestive system, beginning near right kidney, covering anterior half of visceral hump dorsally, finally extending into cavity on outer side of right shell muscle. Gonoduct (gd) opening into right kidney in both sexes. Urogenital opening not greatly enlarged into papillae in female.
Nervous System: Circumesophageal nerve ring of hypoathroid. Cerebral ganglia at bases of cephalic tentacles connected with thick cerebral commissure over buccal constrictor of oral tube in front of buccal cavity. Pleural and pedal ganglia tightly juxtaposed. Connectives between cerebral ganglia and pedal/pleural ganglia also running toward ventral side of buccal mass. Pedal ganglia almost fused with short commissure.
Cerebral ganglia innervating cephalic tentacles, eyestalks, circumoral region (intensively), but not connected by labial commissure. Labial ganglia also absent. Cerebrobuccal connectives arising from ventral sides of cerebral ganglia, extending along lateral wall of odontophore inside lateral protractors. Buccal ganglia lying between radular diverticulum and floor of anterior esophagus.
Pleural ganglia laterally providing nerves to lateral wall of body musculature including columellar muscles. Visceral nerve loop arising from both right and left pleural ganglia. Supraesophageal part of loop passing over esophagus toward anterior limit of ctenidial attachment. Subesophageal part of loop running beneath esophagus, penetrating part of right shell muscle, emerging in right. From supraesophageal and subesophageal ganglia, relatively thick nerve extending toward osphradioctenidial ganglia and mantle margin. Osphradioctenidial ganglia innervating osphradia on inner anterior sides and efferent ctenidial axes on outer posterior sides. Pallial nerves derived from supra-/subesophageal nerves, uniting with nerves from pleural ganglia through zeugoneury. Supraesophageal-visceral connective innervating mid-esophagus by very thin nerves. Subesophageal-visceral connective innervating anterior lobe of right kidney. Visceral ganglion weakly developed between right and left kidney openings beneath rectum; innervation not clearly observed, but at least thin nerves proceeding to both kidneys.
Pedal cords well-developed, connected to several distinct commissures, exhibiting scalariform configuration. Thin anterior pedal nerves extending from pedal ganglia into pedal musculature. Statocysts lying on anterodorsal sides of pedal ganglia.
|