CHAPTER 3
Methods
|
Roentgenological, microscopic histological, and macroscopic gross anatomical examinations were attempted in order to find a method for the diagnosis of osseous syphilis. Furthermore, methods of differential diagnosis and of palaeopathological diagnosis of osseous syphilis in the cranium were also attempted based upon those examinations. 1. Roentgenological Examination (see Plate 1.1-a, b).
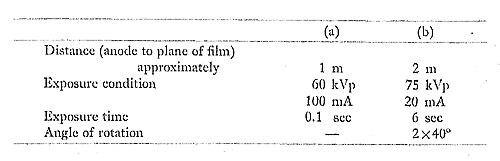
The conventional roentgenograph (a) and tomograph (b) were taken under the following conditions.
The ordinary roentgenograms showed only obscure contrasts of the shadows (Plate 1.1-a) corresponding to the syphilitic lesions, which were easily recognizable on gross observation. Furthermore, the tomographs (Plate 1,1-b) did not show any characteristic signs of osseous syphilis in the skull. It was concluded, therefore, that analyses of the roentgenological features are not the most suitable approach for a differential diagnosis between syphilis and other pathological changes on the cranium such as non-specific suppurative or pyogenic infections. 2. Microscopic Histological Examination (see Plates 2.1 and 2.2)
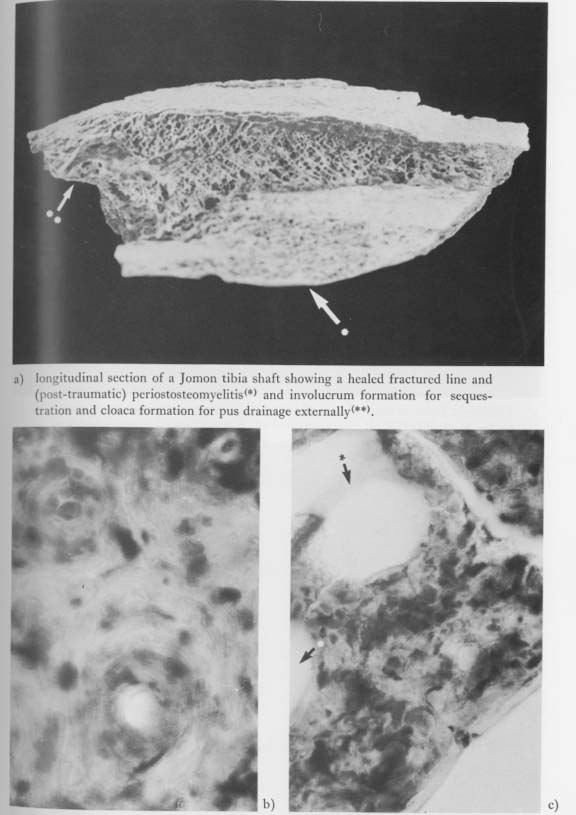
Ground sections of a tibia of the Edo period and of the Jomon period were embedded in plastic before thin slices were cut using a diamond cutter and stained with hema-toxylin-eosin. Microscopic examinations, in a tibia of the Edo period showing irregular swelling of the shaft with bone sclerosis which might have been caused by syphilis, revealed that the Haversian system and lamellae could be well demonstrated and held their structural detail and typical arrangement, at least in the normal cortex region. In the subperiosteal sclerotic region, however, the bone material was more compact than in normal cortex, and there were reactive new bone proliferations accompanying sinusoid spaces sur rounded by comparatively fine lamellae. Such sinusoid formations might have been produced by necrosis in the syphilitic processes (Plate 2.2-a, b, c). The Jomon specimen, on the other hand, a fragment of fractured tibia, was diagnosed as post-traumatic nonspecific suppurative periost-osteomyelitis because of the large cloaca formation for external pus drainage and the narrowing of the medullary cavity by new bone proliferation (Plate 2.2-a). At higher microscopic magnifications, however, the Jomon tibia failed to reveal very clear lamellar structures, probably due to the damage from soil and physical stresses. Neither could osseous lamellae nor canaliculi in the osteomyelic lesions of the Jomon tibia be observed, although large sinusoid spaces surrounded by homogeneous material in the subperiosteal proliferative region (sequestra formation or cloaca) were recognized (Plate 2.2-b, c). GOFF (1967), after having applied all available methods to differentiate osseous syphilis from other pathological changes of bone, particularly in the skull, stated, "Having applied numerous laboratory methods and tests, to have cut, sectioned, polished, stained, macerated and ground bones, the stark limitations of our capacity to prove clearly the presence of syphilis as a causal agent has been frustratingly emphasized to me." On the microscopic study of human costa invaded by syphilis MORSE (1978) stated, "As might be expected, the histological preparation shows a major degree of artifact, presumably because of chemical action in the soil from many years of burial. Never theless, those portions of bone which retained fairly good morphologic characteristic appear quite regular, particularly with respect to the Haversian system. I am unable to state with certainty the nature of the defects in the cortical surface noted grossly, since their margins are badly altered from the long exposure." Thus, neither microscopic nor roentgenological features reveal very much concerning the true differences between various pathological changes, including syphilis and other non-specific periost-osteomyelitis, found in ancient human skeletal remains; and there seems to be no alternative but to wait for further research in this field in the future. 3. Gross Pathology (see Plates 3.1, 4.1, and 4.2)
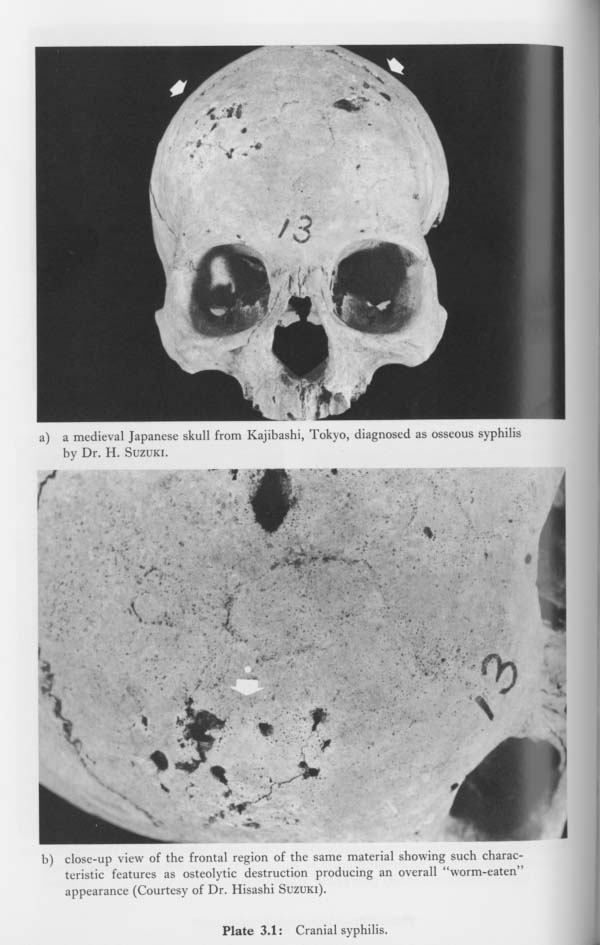
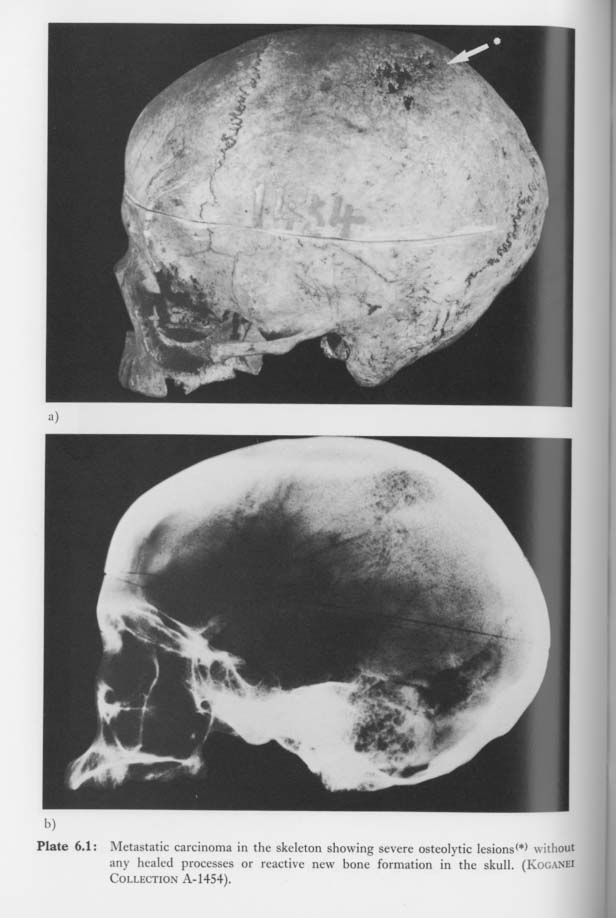
Macroscopic observation provides basic direction for the diagnosis of pathological changes in ancient human skeletons; in particular it provides important information for the differential diagnosis between osseous syphilis and non-specific suppurative periost-osteomyelitis. In general, there is a considerable difference in the frequency of these two diseases in the cranium. The cranium is rarely involved in suppurative periost-osteomyelitis, whereas it is one of the regions most frequently affected by osseous syphilis (see Table 3.1), Dramatic changes spreading throughout the entire cranium are one of the most characteristic features of osseous syphilis.
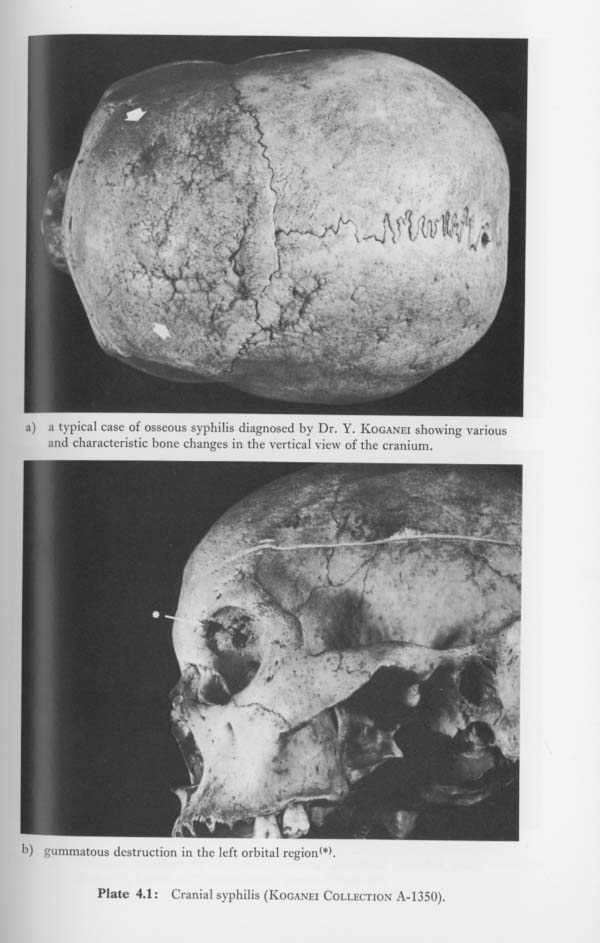
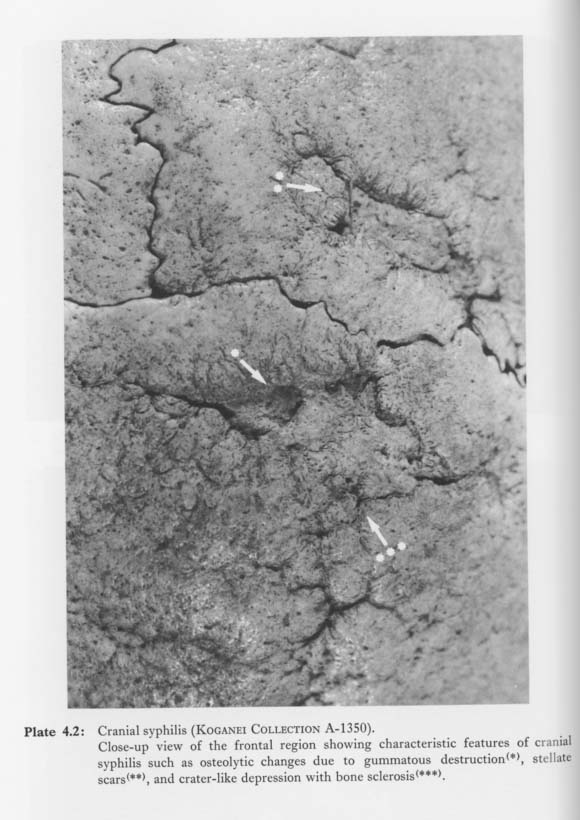
In the long bones, particularly those of the lower extremities, it seems that new bone formation is greater in cases of non-specific infections than in cases of syphilis. Usually new bone formation in non-specific periost-osteomyelitis results in the bone surface becoming more irregular. In pyogenic periost-osteomyelitis, there also seem to be many large cloaca formations for pus drainage and/or large sequestra. On the other hand, features such as sclerotic bone swelling with smooth bone surface or a notable lack of suppurative cloaca and sequestra formation (see STEINBOCK, 1976) are thought to be keys in postcranial syphilis. The foregoing indicate that palaeopathological diagnosis of osseous syphilis in ancient bones is better carried out mainly by macroscopic observation or gross pathology rather than by roentgenological analysis or microscopic examination. With regard to the gross pathology of osseous syphilis in the cranium, a large number of studies have been published since VIRCHOW (1856) first described in detail the morphological changes of osseous syphilis in the skeleton. In Japan, KOGANEI (1894) and SUZUKI (H; 1963) have shown cases of typical osseous syphilis in the cranium and given brief descriptions of their pathological changes (see Plates 3.1, 4.1, 4.2). On the basis of those studies, the author would like to propose three main morpho-patho-logical characteristics of osseous syphilis in the cranium along with the introduction of an excellent example of typical osseous syphilis found in the recent Ainu skeletal remains collected and reported by KOGANEI. This specimen, catalogued as A-1350, is an almost complete skeleton and includes the skull and main long bones, which are preserved in good condition. In this specimen, there were remarkable pathological changes caused by osseous syphilis both in the skull and postcranial skeletons, as pointed out by KOGANEI, Particularity in the skull, diffuse gummatous osteolytic lesions with partial new bone growth are widespread in the frontal bone, in both parietal bones, and in the orbital region (Plates 4.1, 4.2), The morphological features consist of diffuse osteolytic defects, many stellate scars with considerable bone sclerosis, and new bone formation that shows the healing process. There is, however, no clear evidence of syphilitic changes around the nasal and palate regions. As a result of the above-mentioned severe bone changes on the surface of the skull, a wrinkled or worm-eaten appearance exists which is the same as STEINBOCK (1976) has described in many typical cases of cranial syphilis. In the present study, the three main morpho-pathological characteristics (triad) of cranial osseous syphilis in gross pathology are defined as follows: 1. Diffuse and multi-focal lesions: Syphilitic lesions produced by the formation of gummatous areas are usually diffuse and multi-focal over the entire cranium. Pathological erosion due to syphilis begins almost at the pericranium, and extends rapidly and widely over the outer table of the skull (see STOKES, 1927; and STEINBOCK, 1976). 2. Various morphological features: In the gross pathology of cranial syphilis, lesions show such various morphological features as osteolytic destruction, resorptive bone changes, sclerotic clumps of bone, stellate scars, and an overall worm-eaten appearance (STEINBOCK, 1976). These are thought to be most important diagnostic signs of cranial syphilis. Osteolytic perforations through the cranial table, which might be brought about by gummatous destruction and by bone necrosis, are also relatively frequent features in typical cases of osseous syphilis (KOBAYASHI, 1981). Crater-like depressions and/or stellate scars with bone necrosis are also very often recognized in syphilitic lesions 3. Healed processes: Another diagnostic feature of cranial syphilis consists of reactive and irregular new bone formation which usually grows around the margin of the osteolytic defects and sometimes gives the vault a folded or wrinkled appearance. New bone formation may be equivalent to the healing processes in osseous syphilis. It sometimes forms on the surface of the old cortex, appearing rather like a coating of pumice stone when the bone is dry (GOFF, 1967). In this study, the palaeopathological diagnosis of osseous syphilis in the cranium was made on the basis of these three morpho-pathological characteristics. 4. Differential Diagnosis of Osseous SyphilisPalaeopathological diagnosis of osseous syphilis may be carried out with ease in typical cases of human skeletal remains in Japan since, as mentioned before, there appears to have been no non-venereal treponemal infections such as yaws, pinta, bejel, etc., in this country in older times. As is well known, however, it is very difficult to diagnose cases as syphilis if there have been only atypical and minor changes in the bone. In such cases, the lesions often resemble those of other bone pathologies such as non-specific infections and certain kinds of malignant tumors. Naturally, it is necessary to have sufficient knowledge or information concerning osseous syphilis and other bone disorders in the skeleton, particularly in the skull, to be able to distinguish between them. Currently, the following bone diseases should be considered in the differential diagnosis of osseous syphilis from the palaeopathological point of view. 1. Pyogenic periostitis and osteomyelitisPyogenic osteomyelitis may closely resemble the osseous lesions of syphilis in the initial stage of periostitis and ostitis (STEINBOCK, 1976). In advanced cases of syphilis, the long bones, which show predominant sclerotic enlargement or swelling with ivory-like bone weighing much more than normal (GOFF, 1967), are frequently invaded bilaterally. On the other hand, in pyogenic periost-osteomyelitis, the long bones, which frequently show irregular plaque-like formation (STOTHERS and METRESS, 1975), often with suppurative cloaca and sequestra formations, are usually affected on one side only. In addition to these factors, one of the most important points in differentiating osseous syphilis from pyogenic periost-osteomyelitis is the location in the skeleton where the two diseases are most frequently involved. It should be noted that tertiary or osseous syphilis usually involves the cranium. On the contrary, pyogenic infections of the bone, which may cause extensive bone necrosis and large sequestra formations, rarely affect the cranium independently. Careful investigation, of course, may sometimes be required when secondary pyogenic infections derived from other bone pathology occur in the cranium (see GREGG et al., 1982). 2. TuberculosisBecause tuberculosis may often cause skeletal changes similar to those of syphilis in dried bones, it has been emphasized that skeletal tuberculosis should be clearly distinguished from osseous syphilis. Recently STEINBOCK (1976) described the dif ferential diagnosis between skeletal tuberculosis and osseous syphilis as follows: "In the early stages, tuberculosis tends to be progressive with predominant bone destruction. Even in the later stages there is very little new bone production, The hyper-trophic swelling of the long bone diaphyses rarely occurs in tuberculosis compared to syphilis. Tubercular erosion of the cranium is infrequent but usually begins in the inner table instead of the frequent involvement of the outer table by syphilis." In skeletal tuberculosis, the most frequently involved region is the vertebral column (HIRANO, 1958; ITO et al., 1958). On the contrary, tubercular involvement of the cranium seems to be very uncommon. According to statistical observations on bone and joint tuberculosis in 4873 cases by HIRANO (Table 3.2), there was no incidence of cranial tuberculosis. The same lack of occurrence was obtained by ITO et al. KATAYAMA (1962) stated that the most frequently involved site in cranial tuberculosis, although it occurs very rarely, is in the facial region, especially in the infraorbital area.
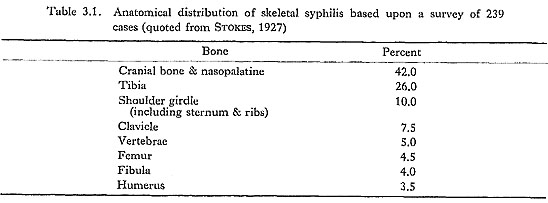
In Japan, from the palaeopathological point of view, OGATA (1972), SUZUKI (T; 1978), and TASHIRO (1982) reported postcranial tuberculosis in three ancient skeletons, but there were no cases of skull involvement. 3. Paget's disease (ostitis deformans)The most common sites of this chronic bone disorder are the pelvis, femur, tibia, and skull. The principal bone change is some degree of thickening, with the denser cortical bone being replaced by spongy bone (BROTHWELL, 1972). In advanced cases, overall thickening and irregularities of the bone surface are commonly seen in the skull, although there do not seem to be any characteristic features such as stellate scars or crater-like depressions as seen in osseous syphilis. Roentgenological examination of Paget's disease indicates a great density and specific mosaic arrangement of bone cells (GOFF, 1967). A diagnosis of typical Paget's disease is an unmistakable conclusion if many bones are involved. Cook (1980) reexamined in detail five prehistoric American Indian skeletons which had been diagnosed as Paget's disease by DENNINGER in 1933. This gross and histological analysis of DENNINGER'S five cases rejected his diagnosis of Paget's disease. Cook con cluded that the lesions, particularly in the cranium, were suggestive of treponemal infection rather than Paget's disease because of the morphological characteristics such as depressed and healed stellate scars and of epidemiological pattern of periosteal lesions as determined by his previous studies on pathological conditions among prehistoric American Indian skeletons. To date, there have been no palaeopathological case reports or discussions of Paget's disease in Japan. 4. Giant cell tumorGiant cell tumors, commonly found in adults in their 20s to 40s, are one of the most common of bone tumors. The most common site involved is the epiphysis of the long bones, especially those of the femur and tibia. The cranium, however, is rarely affected. Giant cell tumors in the long bones may sometimes be confused with the swellings of osseous syphilis. Roentgenograms of this tumor usually reveal a characteristic feature known as "soap bubble appearance" or "honeycombed appearance," which is never seen in the roent-genograms of osseous syphilis. In uncovered skeletal remains, giant cell tumors, although there have been no case reports or discussions of them in this country, would be fairly unmistakable in the skull at least, because there is no characteristic morphology in this bone tumor such as that seen in cranial osseous syphilis. 5. OsteosarcomaOsteosarcoma is one of the most representative primary malignant tumors of the bone. This osteogenic malignant tumor is most commonly found in younger people, especially those from ten to nineteen years of age. Even with the advances of modern medicine, the prognosis for this tumor is very serious (LICHTENSTEIN, 1977). Osteosarcoma comprises about ten percent of all bone tumors, ranking third in frequency among bone tumors in Japan (MATSUNO and GOTO, 1976). The metaphyseal area of the long bones is the major site of Osteosarcoma involvement, and the tumor usually involves a single lesion of the skeleton. The bones most frequently involved are the distal portion of the femur; next, the proximal portion of the tibia; and some-times the proximal portion of the humerus. Osteosarcoma, however, less commonly involves the skull. The gross pathology of osteosarcoroa usually shows severe osteoplastic changes with ossification and calcification, although there are sometimes significant osteolytic changes. The most characteristic feature in dried bone are the so-called "radiating spicules" which are derived from massive and irregular bone apposition. Roentgenological examination sometimes reveals such particular features as "sun burst" or "spicula formation," which are seldom found in cases of osseous syphilis. The large difference in age groupings helps in regard to the palaeopathological differential diagnosis between Osteosarcoma and osseous syphilis. The distribution patterns of the involved bones for these two bone diseases also show considerable differences, i.e., osteosarcomas rarely involve the cranium, whereas syphilitic lesions are frequently seen there; further, this malignant bone tumor usually affects only one side in the long bones, whereas syphilis usually affects the bones bilaterally. 6. Multiple myeloma and secondary metastatic carcinoma of the boneBoth multiple myeloma and secondary metastatic carcinoma of the bone are malignant bone tumors which may often prove difficult to distinguish in the differential diagnosis of osseous syphilis, especially in the skull. These two malignant bone tumors affect older age groups, particularly persons over the age of fifty. The skeletal locations of these malignant bone tumors are relatively similar to each other. Pathological lesions are frequently found in the vertebral column, pelvis, ribs, and skull. These two malignant bone tumors may produce equal osteolytic defects of various sizes in the skull. However, lytic lesions accompanied by sharp and circum scribed edges rarely have the healing processes or reactive new bone growth which are usually seen in osseous syphilis. Particularly in the skull, such characteristic changes of syphilis as reactive new bone growth, necrotic destruction, and stellate scars with sclerosis are never found in the lesions of these two malignant bone tumors. Recently the author (SUZUKI, 1981) investigated a case of multiple myeloma found in a skull of the Edo period from the morpho-pathological and roentgenological points of view, and discussed some problems of the differential diagnosis between multiple myeloma and osseous syphilis (see Plate 5.1-a, b).
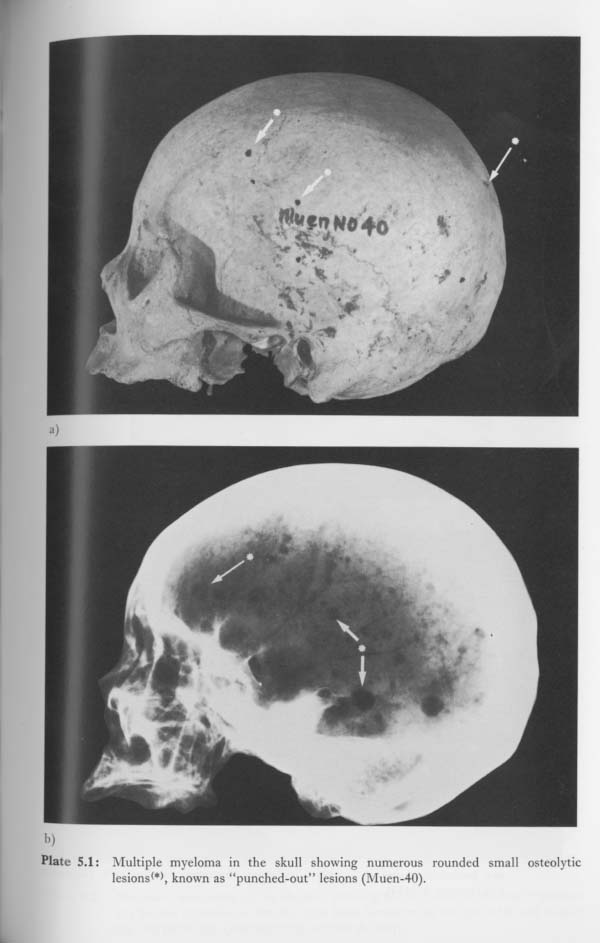
Herein the author will present new evidence with regard to palaeopathological. cases of secondary metastatic carcinoma of the bone in Japan. The skeleton, excavated from Kitami, Hokkaido, is one of the Ainu skeletons collected by KOGANEI and now housed in the Department of Anatomy, the University Museum, The University of Tokyo. The specimen, catalogued as A-1454, was an almost complete skeleton of an adult female with the age estimated at more than thirty years. This individual had remarkable pathological changes on the entire skeleton. Severe osteolytic lesions, which were not described at all in detailed description by KOGANEI (1894), were found in the vertebral column, pelvis, ribs, scapulae, and cranium (see Plates 6.1, 6.2). In the skull, lytic lesions clearly exist in the parietal bone and in the left of the facial bones. Especially in the parietal region, numerous concentrated small rounded lytic defects are evident and seem to form a comparatively large osteolytic lesion as a whole. There is no evidence of healing processes around the lytic defects or any of the lesions.
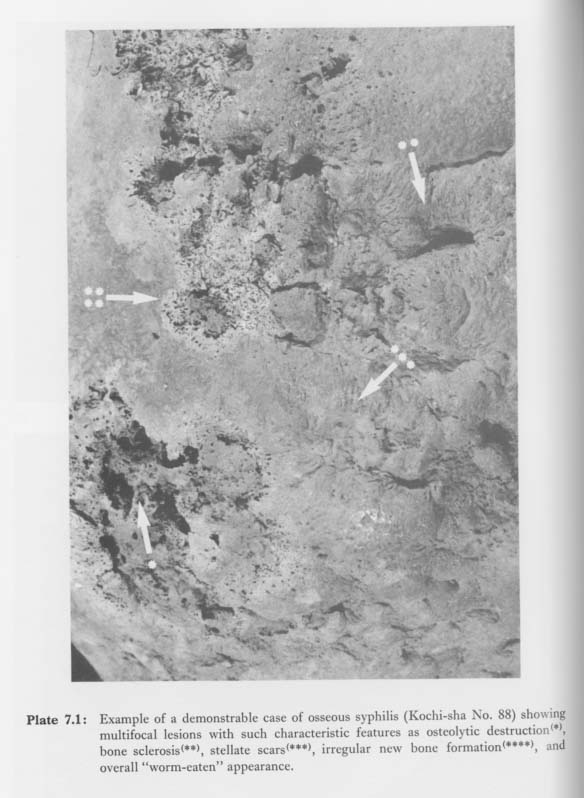
The postcranial skeleton, consisting of the pelvis, ribs, scapulae and vertebral column, also exhibits considerable osteolytic destruction without reactive new bone growth. Roentgenological examination of the skull revealed an obscure and relatively large osteolytic shadow which clearly does not seem to be similar to those of multiple myeloma. In the roentgenogram of multiple myeloma (see Plate 5.1-b), the characteristic feature is reffered to as "punched out shadows" and usually shows rounded shadows of various sizes widely scattered throughout the entire skull (IMAMURA, 1968; NISHIOKA, 1971). The distribution and gross pathological changes of the osteolytic lesions in this Ainu female skeleton are highly indicative of secondary metastatic carcinoma rather than of multiple myeloma or osseous syphilis. 5. Palaeopathological Diagnosis of Osseous Syphilis in the CraniumThrough examinations of cranial syphilis in the 923 adult skulls of the Edo period, it was found that not all cases which were diagnosed as osseous syphilis satisfied the three main characters of cranial syphilis mentioned before. Some had only a depressive lesion with partial sclerosis, others had a slightly isolated osteolytic lesion, and others had only circumscribed reactive new bone proliferations which made the bone surface in the cranium irregular. In this way, the materials diagnosed as osseous syphilis, in fact, represent various pathological bone changes in the skull from simple to complicated or from atypical to typical. Therefore, the diagnosis of cranial syphilis made in the present study should be weighted according to the morpho-pathological certainty of the lesion. According to this weighted diagnosis, the following three classifications were employed for the diagnosis of cranial syphilis. 1. Cases of "Demonstrable" osseous syphilis (Plate 7.1)
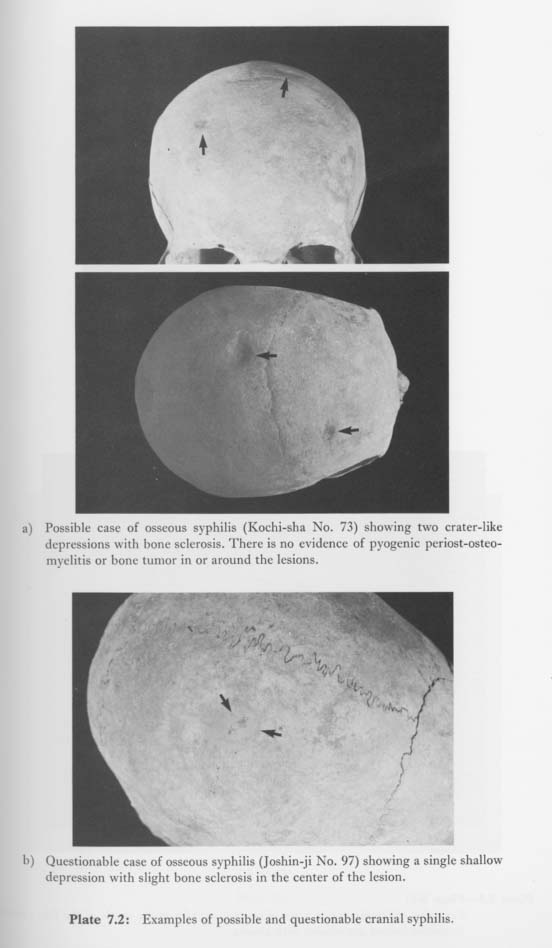
Cases which are diagnosed as demonstrable osseous syphilis should necessarily fulfill the triad of cranial syphilis: (1) diffuse and multifocal lesions scattered throughout the entire skull; (2) various pathological changes such as stellate scars, crater-like depression, necrotic and osteolytic destruction, and bone sclerosis; (3) considerable healing process and new bone formation. Furthermore, cases which show typical gum-matous destruction and deformity in the nasal region, i.e., the "saddle-nose" formation in the facial skeleton, as well as the cases which show apparently syphilitic destruction in the palate are also diagnosed as demonstrable osseous syphilis. Of course, the cases of demonstrable osseus syphilis should certainly be differentiated from other bone diseases. 2. Cases of "Possible" osseous syphilis (Plate 7.2-a)
Cases diagnosed as possible osseous syphilis should usually fulfill at least two charac-teristics of the triad, and should probably be differentiated from the other bone dis-orders listed in the previous section. The pathological changes of these possible cases are necessarily less typical than those of demonstrable cases in gross pathology. For example, a case which shows a single osteolytic lesion surrounded by some sclerotic features coexisting with the healing processes, and which seems neither due to primary pyogenic periost-osteomyelitis nor bone tumors of the skull may be diagnosed as possible osseous syphilis. 3. Cases of "Questionable" osseous syphilis (Plate 7.2-b) Cases diagnosed as questionable osseous syphilis are defined as cases difficult to diagnose with certainty as syphilis. The cranial lesions of such questionable or doubtful cases are, in fact, usually made up of limited and tenuous changes such as single small bone depressions with scant sclerosis, bone surface irregularity without any osteolytic destruction, and shallow pitting with slight hyperostosis on the vault. These tenuous or unstable changes in the skull may occur equally as a result of osseous syphilis or of many other bone disorders. Hence, in the strict sense, in questionable cases it cannot be determined with confidence whether their cranial lesions are caused by syphilis or other pathological bone changes. Consequently, in the present study, the demonstrable and possible cases were used in the statistical approach. Furthermore, only the demonstrable cases, which are of course the most reliable of the three categories, were used in the most sensitive statistical problem, i.e., in the palaeoepidemiological estimation of the prevalence of syphilis among the people of the Edo period. |